

Why do people detransition?
A new paper from the DARE study describes the various internal, external, mental health-related, and social factors for detransition-related decision making. Link provided to access 50 free copies!


Published in the Journal of LGBTQ+ Mental Health, the latest paper from the DARE study presents reasons impacting detransition-related decision-making among a sample of 957 LGBTQ2S+ people.
This link provides the first 50 clicks free access to the article.

The title of the paper
“Gender fluidity and detransition: Results of a cross-sectional online survey of sexual and gender minorities living in the US and Canada”
DARE stands for: detransition analysis, representation, and exploration. It is among the largest community-engaged research project that was ever specifically designed to study gender fluidity, detransition, and retransition. Survey data from 957 US-Americans and Canadians were collected between December 2023-April 2024, (so bear that in mind that time lag when interpreting the results).
From its study design, to results, it finds that detransition is multi-dimensional, complex, and in need of data-driven care and LGBTQ+ community recognition and support.
Who took the survey?
Like all research on detransition and gender fluidity conducted since 2020, it includes a large majority racially-white people born female, most of whom are sexual minorities (bisexual or lesbian), and/or transmasculine. Nearly half the sample affirmed a current trans/nonbinary identity, while the rest were cisgender, detrans, or unsure about gender identity. A large majority (74%) were living in the United States, and respondents had an average age of 26 (a majority were under the age of 29).
100% had initiated some kind of transition (social only, or medical only - social+medical was the most common pathway);
65% had medically transitioned.
The reasons for detransition/retransition included multiple factors and pathways:
A previous paper presents a more fine-grain analysis of four different classes or “types” of detransitions. It shows subtle profile differences across reasons to detransition, broken down by sex/gender, mental health, age of realizing a trans identity, sexual orientation identities, ACEs scores, decisional regret, timelines, and so forth. Access:
A groundbreaking analysis of four detransition types

A long awaited article has just been published in the Archives of Sexual Behavior: “A Latent Class Analysis of Interrupted Gender Transitions and Detransitions in the USA and Canada.”
For the present study (which is more generally descriptive) our team submitted it for peer review in August 2024! While our aim was to have this paper out before the Latent Class Analysis (above), the Gods of Peer Review had other plans for us. Instead, it was first rejected by one LGBTQ+ care journal before it went under review with a second journal in December 2024. After being reviewed by SIX peer reviewers, it was finally accepted.
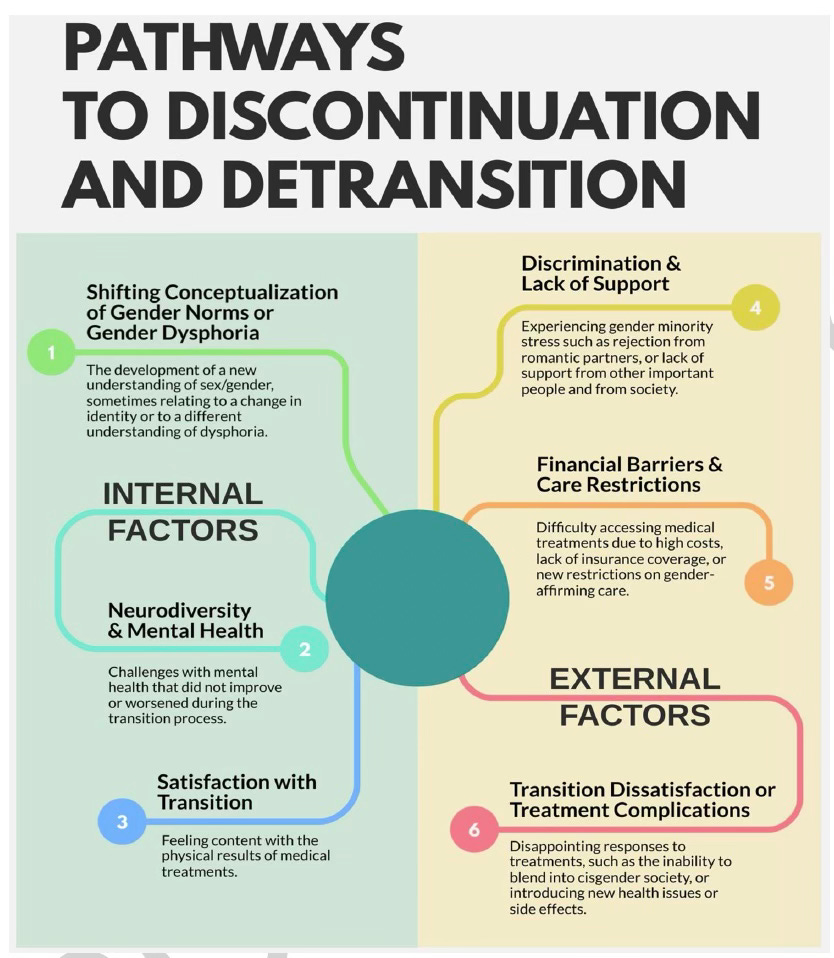
So, what is new and unique about the “Gender Fluidity and Detransition” analysis (compared to the Latent Class Analysis)? It shows descriptive stats from the sample demographics. It also presents Likert scale results, underscoring the strength and proportion of 21 different factors for detransition endorsed by the sample. These reasons range from physical/mental health, to changes in beliefs about gender norms, satisfaction or dissatisfaction with treatments, discrimination and gender minority stressors, loss of access to gender-affirming treatments, re-conceptualizing gender dysphoria as related to something else, and feeling that health did not improve or worsened during transition.
The most commonly reported reason for detransition endorsed in the DARE study are as follows:
Shifting conceptualization of gender and gender norms (52%)
Changes in identity (47%)
Lack of mental health improvement while transitioning (40%)
Gender dysphoria resolving over time (41%)
Discrimination (39%)
Realizing that gender dysphoria was caused by something specific (i.e. trauma, abuse, autism) (39%)
Continuing to be perceived as transgender (i.e. not “passing”) (31.7%)
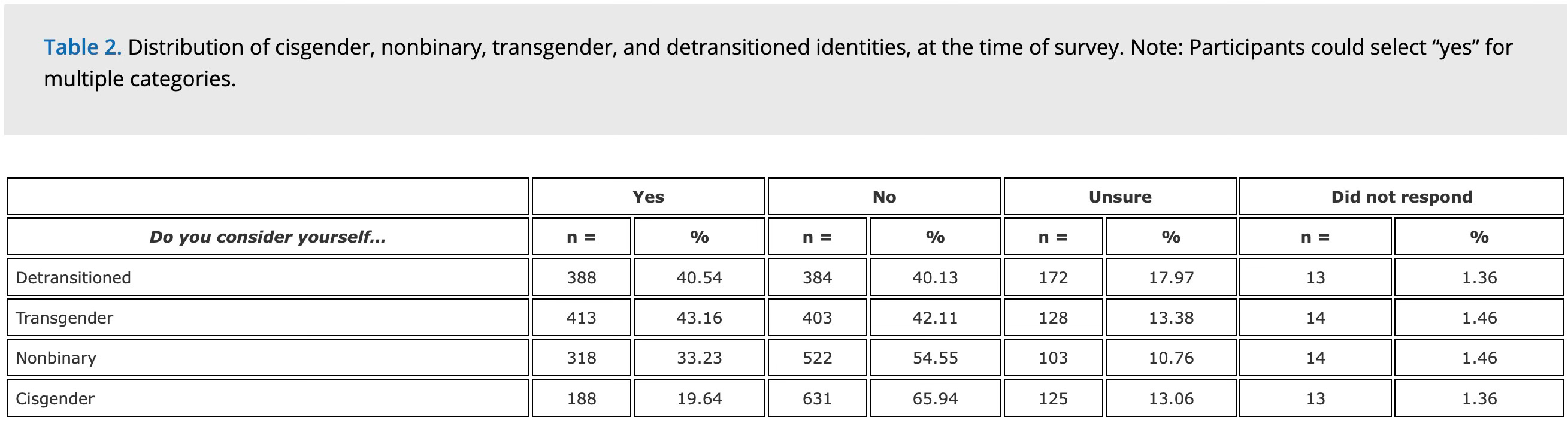
One of the strengths of the study is that it includes a mixed demographic of folks who currently affirm a transgender or nonbinary identity, as well as many who no longer understand themselves as trans or gender-diverse. A substantial portion consider themselves “unsure” on current trans/detrans/cisgender status, which is relatively common for people in a detransition process.
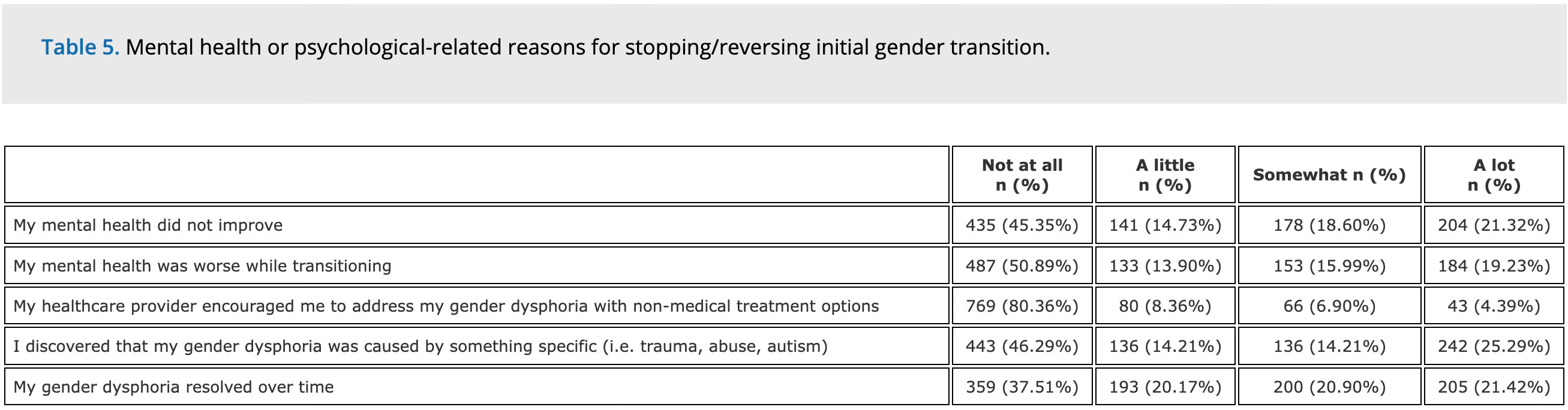
There are multiple Tables presenting the various reasons why people decided to detransition, so check out the paper to see all of them (it’s worth looking at!). Here are the ones related to mental health and neurodivergence, structural and gender minority stressors, and identity-related or shifting beliefs:
To triangulate some of the above, we looked at participants’ Adverse Childhood Experiences (ACEs) scale items. (71.47% completed this questionnaire). The mean ACE score was 4.03 (range 0–11). The most commonly endorsed ACE items were exposure to emotional abuse (n = 747, 78.01%), living with someone with mental illness or suicidality (n = 641, 66.98%), and physical abuse (n = 422, 44.10%). This is substantially higher than global population estimates (mean ACE = 1.79) found in a large-scale meta-analysis of over half a million adults across 22 countries (Madigan et al.). In that same meta-analysis, only 16.1% of the general population reported 4 or more ACEs. These findings extend literature indicating that LGBTQ+ and neurodivergent populations report elevated exposure to childhood adversity (Ellis et al., 2021; Petruzzella et al., 2023; Schnarrs et al., 2019).
Autism was also frequently reported: 25.08% reported receiving a formal autism spectrum disorder (ASD) diagnosis by a healthcare professional, and 42.42% identified as autistic or reported ASD self-diagnosis.
Relatedly, a recent study using Swedish healthcare administrative data that found bisexual/pansexual AFAB participants were more likely to receive a neurodevelopmental diagnosis and treatment (ASD and ADHD) compared to heterosexual AFAB individuals—particularly during late adolescence (13.6% vs 3.6%; Bränström & Pachankis, 2025). Although potential interactions between neurodivergence and gender/sexuality fluidity are currently unknown, our sample showed a higher prevalence of autism than is typically reported in TGD clinical samples (11%, per Kallitsounaki & Williams, 2023). Consistent with recent community-based studies (e.g., Adams et al., 2025; MacKinnon, Jeyabalan, et al., 2024), we also found high rates of self-identified autism (42.42%), with 12% of participants reported receiving a formal ASD diagnosis after beginning to transition.
Our findings point to a need for greater access to mental health, peer and community supports because a significant portion of the sample strongly endorsed worsening mental health during transition prompting their decision to detransition.
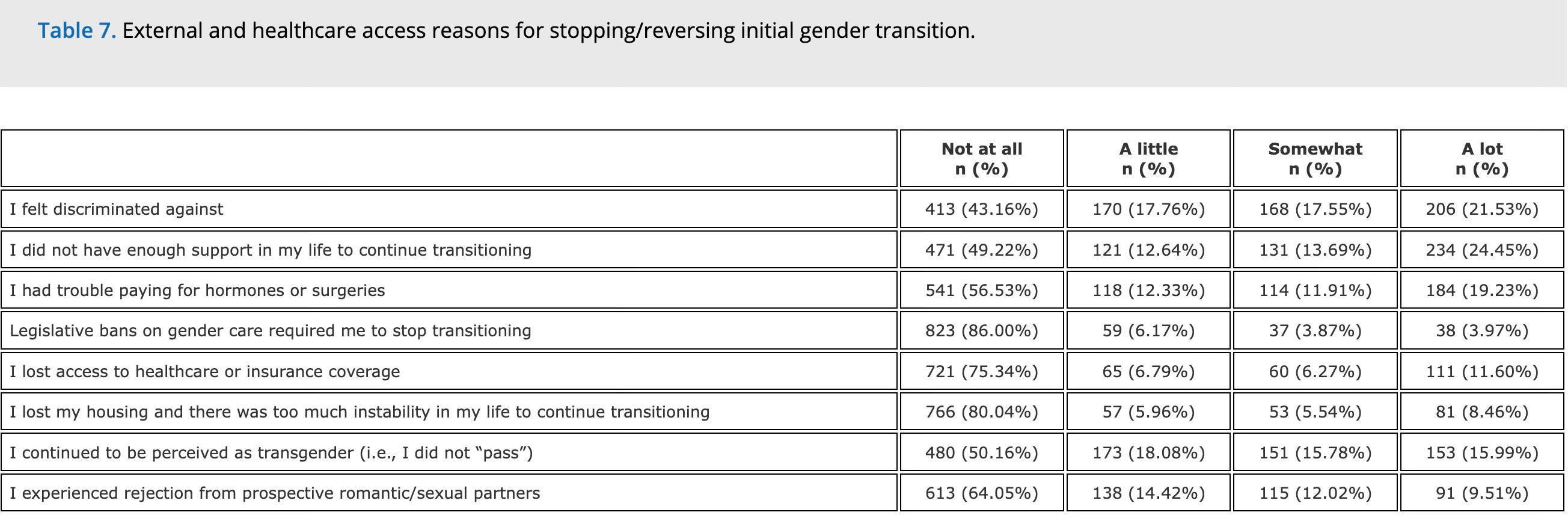
Structural and external factors, such as discrimination or not having enough affirming supports, or lack of access to gender-affirming care were also strongly and frequently endorsed reasons to detransition.
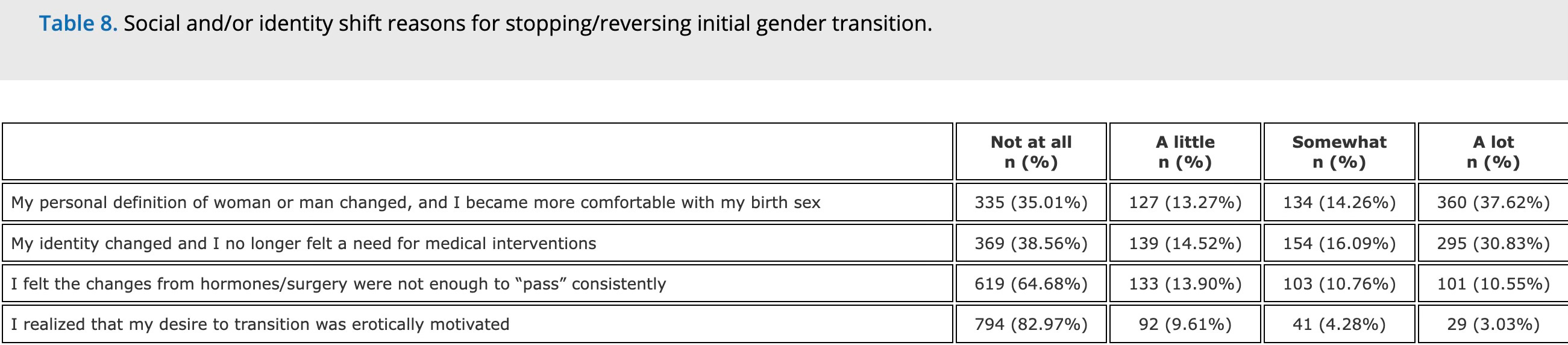
Internal factors, including changing conceptualization of ideas about gender, identity shifts, resolution of gender dysphoria, and feeling that mental health did not improve (or worsened) while transitioning the most frequently and strongly endorsed reasons.
These findings underline prior research from Vandenbussche (2022) which found significant internally-driven detransitions, as well as Turban et al. (2021), that showed social pressure to detransition were predominant factors. Together, the literature reflects intersecting and multi-dimensional influences.
Conclusion
Detransition is shaped by a mix of internal factors—such as changes in identity, evolving beliefs about gender, or unmet expectations from medical treatment, neurodivergence and autistic identity development, and external factors, like discrimination or lack of support. By including a broader range of participants than earlier detransition studies, the DARE study captures more varied and diverse experiences.
The study also highlights that some people stop medical treatments not out of regret, but a wider range of emotions and experiences of transition. About a third of the sample stopped treatment because they were satisfied. About half the sample reported decisional regret with having taken hormonal treatments or had surgery (greater regret was reported with surgery).
One of the key contributions of this paper (please read the full article!) is contextualizing the results with broader findings coming out in LGBTQ+ youth research showing surprising gender fluidity that was not anticipated years ago.
Substantial gender identity/expression fluidity characterized this sample. Participants reported a lifetime average of 4.22 lifetime gender identity/expression labels (e.g. trans man, nonbinary, genderqueer, gender nonconforming, man, woman, etc). 42% reported discontinuing and later resuming transition (e.g., “retransition”). Gender fluidity alongside plurisexual orientations (e.g., pansexual, bisexual, and/or queer), suggests potential interactions with gender and sexuality exploration in adolescence–a pattern consistent with other recent research (Katz-Wise et al.).
The broader research pointing toward gender identity fluidity is paradigm shifting.
After decades of a clinical and media landscape ushering in notions of “born this way,” transnormativity, and “the true gender self,” the DARE study results should be understood within the broader context of gender fluidity at 18% to greater than 50% among trans/nonbinary/detrans populations. The fluidity being observed here also related to LGBTQ+ identities in particular, and especially among those born female.
This is a topic that Pablo and I are currently writing about in our forthcoming book. An update on the book project is in store in the weeks to come! Stay tuned for more from us.
 | A guest post by
|
I feel like there should be different terms for when people desist medical intervention and/or go back to pretending to be the wrong gender due to external factors and for when people realize that they were actually on the wrong track for themselves to begin with…
Like those are just two entirely different things.
great article